


Male Pattern Alopecia
Clinical Presentation(1, 3)
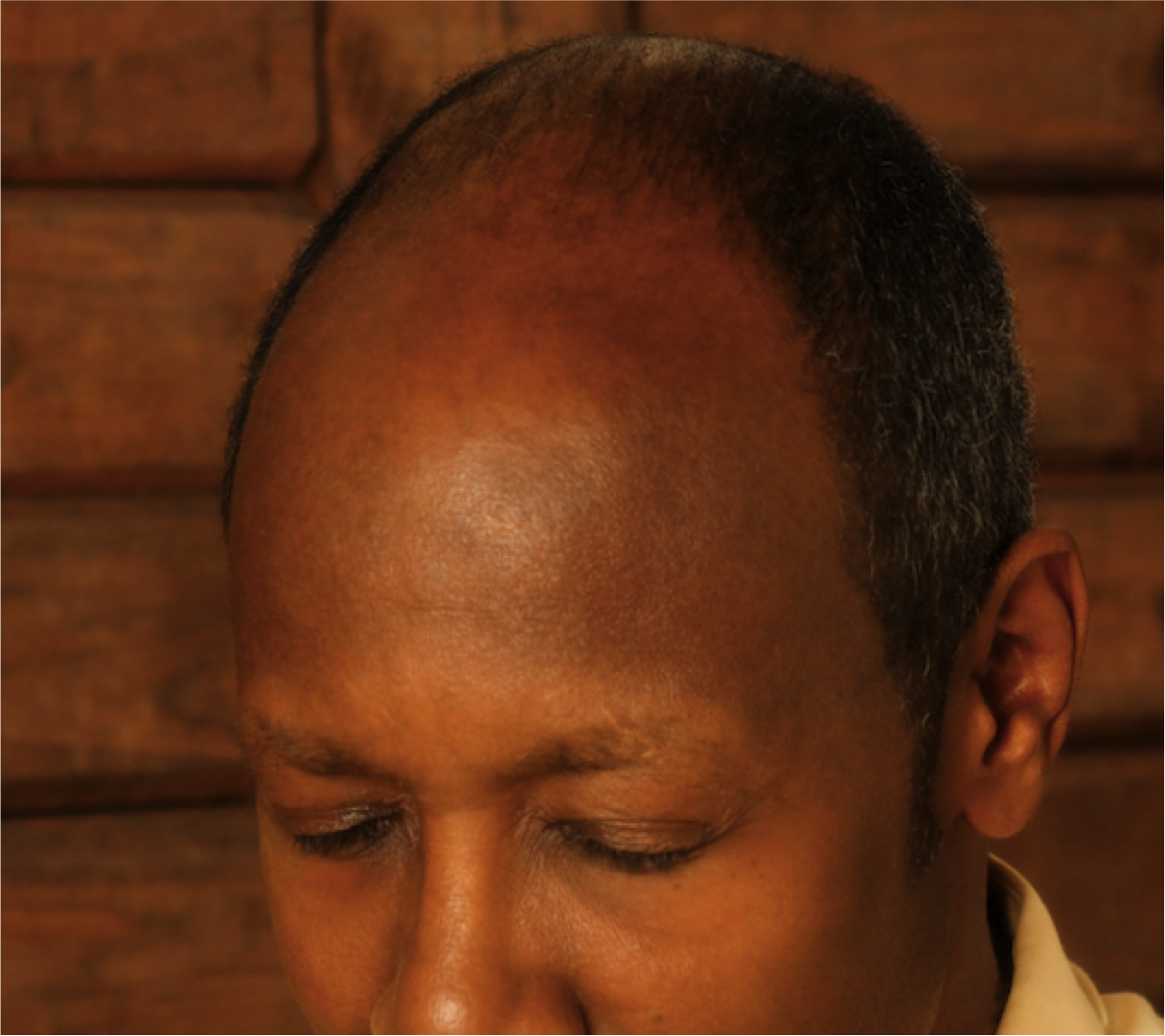
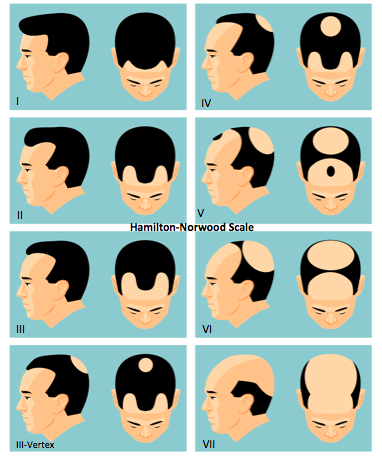
Male pattern alopecia (MPA)/ androgenetic alopecia is a chronic progressive non-scarring hair loss condition occurring in a pattern. Frontal, temporal, vertex scalp are commonly affected and deep recession of the fronto-temporal hairline is seen. Hair thinning may lead to complete baldness in affected areas. The Hamilton-Norwood scale is used to classify the progression of the disease.
Epidemiology(1)
Most common hair loss disorder affecting men. Affects up to 80% of Caucasian men by the age of 70 .
Causes (2)
There are several proposed mechanisms for MPA including:
Genetic predisposition
Hormone abnormalities (hair follicle): Androgen sensitivity and increased production of dihydrotestosterone (DHT) in the follicle leading to miniaturization (hairs shrink in size over time to small, thin, short vellus hairs, eventually leaving a bald scalp) in the genetically susceptible follicle. Increased numbers of telogen (resting) follicles and shorted anagen (growth) phase are also seen in MPA.
Diagnosis (1, 3)
MPA is diagnosed via history, clinical scalp exam, and dermoscopic evaluation. Rarely, scalp biopsies are performed to confirm the diagnosis.
Clinical Imitators (Differential Diagnosis) (1, 3)
Alopecia areata, lichen planopilaris, central centrifugal cicatrial alopecia, telogen effluvium
Associated Conditions (2)
Metabolic disease (insulin resistance, cardiovascular disease) (2)
Treatment Options (1, 2, 3)
Treatment (single or combination) depends stage/ extent of the condition.
Anti-androgens: 5-alpha reductase inhibitors (reduces DHT- oral finasteride, dutasteride), topical ketoconazole
Post Finasteride Syndrome (4, 5):
Definition: “An array of sexual side-effects (decreased libido, erectile and ejaculatory dysfunction and gynecomastia), but also depression, cognitive impairment, fatigue, and suicidal ideation, among others, directly related to finasteride use that persist or commence after discontinuation of
the drug” (4)
The existence of this syndrome is under debate and requires extensive further study (6)
The true prevalence is unknown
Growth stimulants: Minoxidil (anagen phase promoter- topical)
Phototherapy: Low level light therapy
Hair Restoration: Platelet rich plasma, hair transplantation
Scalp camouflage: Scalp micro-pigmentation, hair fibers, color stick, and scalp prosthesis (e.g. customized wigs).
Essential oils: rosemary essential oil (7)
Nutritional supplementation